



30 obstetric clinicians were trained to undertake advanced obstetric care including major surgery, such as Caesarean section and vacuum delivery. One failed 2 final examinations. Of the 29 who qualified; 1 died; 1 left after undertaking 5 years of advanced obstetric care. Twenty-seven are currently clinically active as obstetric clinicians.
17 neonatal clinicians were trained to undertake advanced neonatal care. One left immediately after undertaking the final examination and emigrated to the USA. One became ill but is currently planning to join a hospital. One joined the MOH and is Liberia’s Lead Trainer of neonatal clinicians in Liberia. She is clinically active in caring for newborn infants in different hospitals. 15 are, therefore, working as neonatal clinicians in hospitals in Liberia.
12 paediatric clinicians were trained to undertake emergency care of children. One failed 2 final examinations. 11 are working as paediatric clinicians.
12 obstetric clinicians achieved distinction in their final examination, and 8 achieved a merit. 6 neonatal clinicians achieved distinction and 5 a merit. Among 12 paediatric clinicians, there were 3 distinctions and 5 merits.
-
(1)
The training of obstetric clinicians
Nine Liberian obstetricians, with extended visits from 8 international obstetricians, supported the training. Later, 9 qualified obstetric clinicians also contributed to training and helped to train qualified Liberian doctors who were interested in becoming obstetricians.
Apprenticeship involved the performance of essential obstetric procedures and the management of major complications of pregnancy and delivery under the supervision of the trainers. Trainees progressed from assisting with procedures and emergency management, through to direct and indirect supervision, and finally, being able to manage emergencies and perform procedures independently. Surgical procedures included complicated caesarean sections, and management of ruptured ectopic pregnancies and miscarriages. Towards the end of training, there was close involvement with Liberian doctors in learning to undertake emergency hysterectomy as a last resort to save lives, where standard treatment of obstetric haemorrhage has failed.
Common to many low resource countries, a large proportion of pregnancies in Liberia occur in adolescents under 18 years of age [23]. Many in Liberia are delivering babies when under 16 years of age (Personal observations Professor Southall and [23]). Apart from the well-known risks they face related to their pelvic development, their psychological and emotional needs required a compassionate approach [24]. Throughout our training, the special needs of adolescent pregnant girls were emphasised.
The first two trainee obstetric clinicians began their training at CB Dunbar Hospital in October 2013 and qualified in 2016. A film and report about the onset of the Liberian task shifting obstetric clinician program is linked to in Table 1.
The Ebola outbreak from 2014 to 2016 disrupted the supportive training by international experts, but the obstetric clinician trainees continued to work throughout the outbreak, providing much needed support to the lead Liberian obstetrician.
These first two trainees passed their end of second year OSCE with high marks (81% and 76%) and in October 2016 qualified. They were licensed to practice by the LMDC and were contracted to work as obstetric clinicians in public hospitals chosen by the MOH. In addition to CB Dunbar Hospital, they worked in 3 additional hospitals (Phebe, CH Rennie, and Redemption). They assisted in the training of junior doctors and participated in the management of all activities within the maternity unit. They shared the heavy workload with those doctors who were present. Their work, particularly overnight, helped to provide better sleep patterns for all. They substituted for doctors, both junior and senior, during night shifts. In most rural hospitals at this time there was usually only one senior doctor (not always having had obstetric training) and no junior doctors. Addition of qualified obstetric clinicians created an efficient working environment that helped to create a safer and more effective system. (Personal observations Dr Dolo and Professor Southall).
From the start of the apprenticeship part of their training in October 2013 until March 2015, both trainees helped perform 353 advanced obstetric procedures, including 236 Caesarean sections [25]. They also helped manage 41 patients with eclampsia or severe pre-eclampsia, 25 with post-partum haemorrhage and 21 with shock
A further 7 midwives and 2 physician associates with obstetric experience began their training in October 2015. By February 2018, all trainees had passed their end of 2nd year OSCE and all but 1 (a physician assistant) performed well in their weekly exams.
They began their 3rd year of training in 4 rural hospitals, where they worked in partnership, as interns with local doctors to care for pregnant patients. They also worked closely with community midwives to enhance the integration necessary to reduce delays in recognising, treating, and referring patients.
By April 2019, a final examination, both written and oral, was undertaken. This included caesarean section (basic and complicated) and abdominal operations such as ruptured ectopic pregnancy. The oral examination included management of catastrophic haemorrhage and obstructed delivery as well as the emergency treatment of eclampsia and life-threatening infection. It also addressed the management of fetal distress and the prevention of stillbirth and birth asphyxia. Eight of the 9 trainees were identified as fully competent in the medical and surgical management of critically ill patients. Despite additional training, 1 of the 9 (a physician assistant) continued to fail final assessments, and therefore, 8 of this group of 9 trainees were registered with the LMDC.
From the start of training in October 2013 to the beginning of November 2017, 1,654 Caesarean sections had been undertaken by the first 11 qualified and trainee obstetric clinicians.
The Partnership appointed in January 2018, ten further trainee obstetric clinicians (out of 26 candidates). They were selected from the most remote rural areas of Liberia. These 10 trainees followed the same training plan as the previous trainees and all but 1 successfully qualified in January 2021. This latter candidate, after a further 1 year of training, successfully passed final oral and written examinations in 2022.
Table 1 provides results of the final examination for latest group of 9 obstetric clinicians in September 2023.
Two obstetric clinicians were assigned by the MOH to busy public hospitals (Table 2 hospitals 5 and 6 ) in extremely poor catchment areas in Monrovia (the capital). These assignments followed requests from the doctors working there concerning their high workloads and the high quality of the assigned obstetric clinicians.
Table 1 contains details of obstetric emergency hospital care in 7 hospital and CEmONC facilities in 2021–2022. These data were obtained from the theatre records book only and individual cases have not been further investigated. Its purpose is to give an overview of the emergency obstetric surgical procedures performed. The focus is on the lead surgeon for the procedure and the team is separated into whether the surgery was undertaken by a doctor or an obstetric clinician. The results demonstrate the high load of major operations undertaken by obstetric clinicians compared with doctors.
Table 1 contains clinical reports by 2 trainee obstetric clinicians and one qualified clinician concerning their work
Legend to Fig. 1. Two obstetric clinicians undertaking an emergency Caesarean section at Redemption Hospital (one of the two training hospitals in Liberia).


Two obstetric clinicians undertaking an emergency caesarean section
The progress of every individual trainee was monitored by the recording of each procedure performed and the outcomes during their training, in both a paper and electronic logbook (Fig. 2).

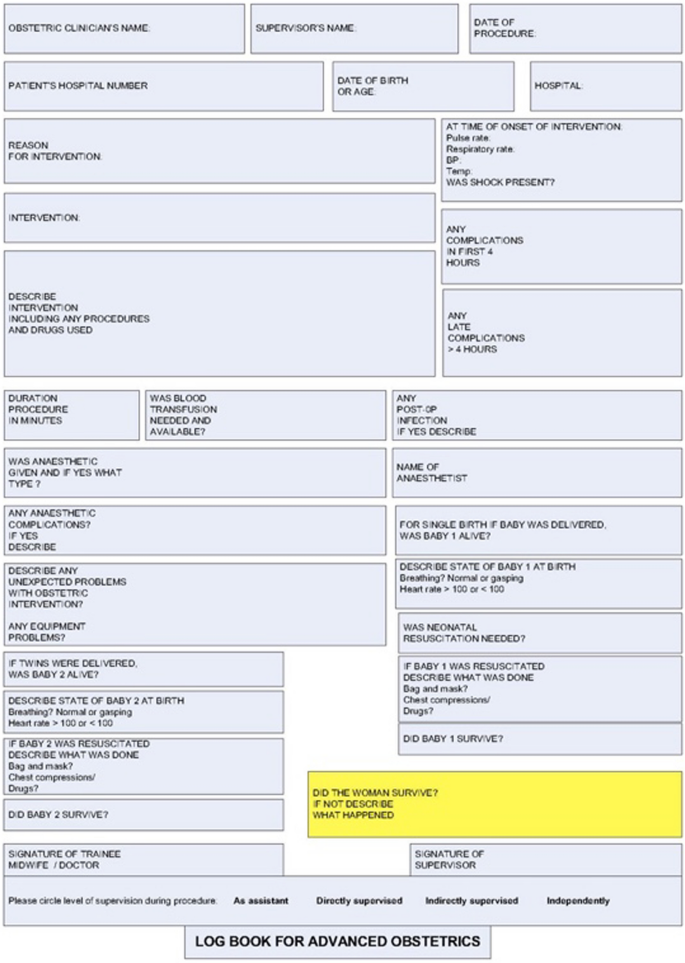
Logbook completed by each trainee obstetric clinician
Legend to Fig. 2. A page of a logbook completed on every patient cared for by each obstetric clinician and subsequently collated at the end of the training.
Table 1 shows the completed and collated logbook of one of the obstetric clinicians through to the end of her training.
-
(2)
The training of neonatal clinicians
This involved supervised work in the neonatal unit, the delivery rooms and post-natal wards. Following resuscitation training, a clinician attended every birth, where fetal distress had been identified. Training was based on the same structure as the obstetric program. However, as no surgery was involved, the training program could be completed in 2 years.
Apprenticeship training was supervised by an international advanced neonatal nurse practitioner. There were regular visits (1–6 months in duration) from MCAI volunteers; a UK ANP, a USA paediatrician and two UK paediatricians.
There was a major emphasis on skin-to-skin care to prevent and manage hypothermia. Suitable harnesses were made in Liberia (see Table 1).
Trainees completed training in neonatal intensive care to WHO level 2. This included nasal Continuous Positive Airway Pressure (CPAP), but not assisted ventilation following intubation.
Rural units, such as Martha Tubman Memorial Hospital unit in Grand Gedeh county, are now managed and led by 2 qualified neonatal clinicians (Table 2). Around 45 critically ill newborn infants are treated in this Hospital every month.
Table 1 illustrates the Admission, Progress and Discharge Forms completed on all admissions.
Monitoring and evaluation required that each trainee record all performed care and the outcome in a paper and electronic neonatal clinician logbook (Fig. 3).


Logbook completed by each trainee neonatal clinician
Legend to Fig. 3. A page of a logbook used by neonatal clinicians to document the management of every newborn infant they cared for and subsequently collated at the end of the training.
Table 1 shows the completed and collated logbook of one of the neonatal clinicians through to the end of her training.
Table 1 describes results of the weekly examination for the neonatal clinician trainees in August 2020.
The reason for admission, length of stay and mortality data in the 2 largest neonatal units (CB Dunbar and Martha Tubman Memorial Hospital) for the years 2021 and 2022, are shown in Table 1. The greatest number of deaths resulted from birth asphyxia, followed by prematurity. This is in keeping with international data for causes of neonatal mortality in LMIC [26].
Table 1 presents the final examination results for the latest 8 qualifying neonatal clinicians in September 2022.
Table 1 describes a trainee neonatal clinician’s experience in caring for a newborn baby in the CB Dunbar neonatal unit.
-
(3)
The training of the first 12 paediatric clinicians
Paediatric training was undertaken by a full time international advanced nurse practitioner (ANP) who had worked for many years with Medicine Sans Frontiers in Nigeria. He was supported by two Liberian doctors and nine senior UK paediatricians. All training occurred in Phebe Hospital and began on March 1st, 2022.
Table 1 describes the renovations and new equipment provided for this training.
link