

Introduction
Globally, tremendous progress in child survival has been made over the last three decades. Under-five child deaths decreased by 58 percent between 1990 and 2018, from 12.5 million to 5.3 million. Almost half (2.5 million) of these deaths were classified as neonatal deaths, occurring in the first 28 days of life, showing the high burden of child mortality at this early age (1).
Neonatal mortality varies greatly across geographical regions and is mostly concentrated in low and middle-income countries. In Sub-Saharan Africa and Southern Asia, the average neonatal mortality rate (NMR) ranges between 25 and 28 per 1,000 live births, whereas in Europe, Northern America, Oceania, and Eastern Asia the NMR ranges between 2 and 4 per 1,000 live births (1). In Southern Asia, between 2015 and 2018, almost 1 million newborns died each year, with the neonatal death proportion among under-five child death increasing from 46% in 1990 to 62% in 2018, which is the highest proportion of deaths in South Asia compared to other regions of the world (1). For Bangladesh, NMR has increased to 30 in 2018 from 28 in 2014; which led to an increase of neonatal death proportion among under-five child deaths from 61% to 67% during the same period (2, 3).
A neonatal death surveillance in four districts of Bangladesh in 2016 reported that the leading cause of neonatal death was birth asphyxia (43%), followed by infections (29.3%), and prematurity (22.2%). Day-wise disaggregation showed that 63.4% of newborns who died on their birthday died due to asphyxia, whereas infections were the main cause of neonatal deaths among newborns who died between days 1–6 (48.8%) and days 7–28 (57.5%) (4). Other studies in Bangladesh and similar contexts reported similar causes and trends (5–7). Early identification, treatment and/or referral of these major causes of newborn deaths are essential to reduce neonatal deaths, especially infections, which are better managed by a qualified provider when identified and referred early (8–10).
In low and middle-income countries (LMICs), several interventions implemented around the time of birth have been proven effective in reducing neonatal mortality. These interventions are delivered through an integrated community and health facility platform (8, 11, 12). Domiciliary services by health workers’ home visits, birth preparedness education, newborn care practices, identification of newborn danger signs, and early care-seeking have been proven effective to reduce neonatal mortality (8, 11–14). However, caregivers’ timely identification of neonatal danger signs and subsequent care-seeking from qualified health providers should be the core of a successful healthcare intervention for neonatal survival (14).
Care-seeking behavior for sick newborns remains low and is a key challenge to reduce neonatal deaths in LMICs (14). This is further compounded by slow recognition of danger signs and delayed care-seeking, as the health condition of sick newborns declines rapidly and can quickly progress to death (15, 16). Care-seeking behavior is a complex decision-making process (17). Multiple factors (i.e., illness severity perception, maternal and newborn factors, health care utilization practices, socio-economic and cultural factors, geographical location, quality of care, cost of care, etc.) influence the caregivers’ and family members’ care-seeking behavior for neonatal illness (14, 18–21).
In-depth understanding of care-seeking behaviors for newborns with danger signs would help to design effective interventions at both community and facility levels (19, 22). There are limited data and studies on newborn illness care-seeking practices in Bangladesh. Earlier studies in Bangladesh investigated the direct relationship of predictor variables with care-seeking practices but did not explore the inter-relationship among the predictor variables (21, 23–26). The most important or influential predictor variables on neonatal care-seeking behavior can be identified through analysis of the inter-relationships among predictor variables and their association with the main outcome variable. This nuanced understanding of important predictors of care-seeking can be used by policy makers, program managers and researchers to inform the design and testing of interventions to improve care-seeking behavior for sick newborns.
Structural Equation Modeling (SEM) has been widely used to simultaneously estimate and test the effects of variables and their inter-relationships within the complex hypothetical conceptual framework (27–30). It allows identification of the pathways of cause and effect from distal factors to proximate factors and to the outcome of interest. Generalized Structural Equation Modeling (GSEM) is the extended and generalized form of SEM for the estimation and testing the effects of categorical, continuous and count variables (31). We used GSEM to explain the relationships among predictor variables in determining mothers’ care-seeking behavior. We also conducted a mediation analysis to estimate the direct, indirect (mediated), and total effects of predictors on the main outcome among each possible mediated pathway found significant in the GSEM analysis (32, 33).
We include the description of the hypothesized conceptual/theoretical model of the inter-relationships between the predictors and the neonatal care-seeking outcome in the next section. Our research objective is to examine this hypothetical inter-relationship with GSEM and identify the most important predictors that have both direct and indirect relationships among them and with the outcome variable. We also estimated the direct, indirect (mediated), and total effect of the predictor variables on neonatal care-seeking.
Materials and methods
Study design, setting, source population and study population
This was a population-based cross-sectional baseline survey conducted in 14 districts (Noakhali, Feni, Chandpur, Lakshmipur, Brahmanbaria, Habiganj, Manikganj, Faridpur, Madaripur, Kushtia, Kishoreganj, Natore, Rajbari and Bhola) that are part of the evaluation of MaMoni Maternal and Newborn Care Strengthening Project (MNCSP) and included both intervention and comparison districts. The MaMoni MNCSP project was implemented in 10 intervention districts out of 64 districts in Bangladesh. MaMoni MNCSP was a United States Agency for International Development-funded project (2018–2023) focused on strengthening public sector maternal and newborn care (MNC) services through increased and equitable accessibility and utilization of quality MNC services in Bangladesh. The key intermediary objectives of MaMoni MNCSP were to advance health system responsiveness, improve MNC service quality and governance, access and demand for services and healthy household practices, and strengthen national capacity to deliver these services with quality at scale. MaMoni MNCSP was implemented by a consortium of local and international partners led by Save the Children. Details of project interventions, project evaluation design, and study settings are available elsewhere (35). As a MaMoni project consortium member, icddr,b conducted the cross-sectional baseline household survey to measure population level coverage of key maternal and newborn practice indicators. The source population was the recently delivered women (RDW) who gave birth within the last 15 months irrespective of birth outcome status in the above-mentioned 14 districts. The study population of RDW was selected from the source population with the sampling techniques described below.
Sample size, sampling and study subjects
The sample size was primarily calculated to detect the minimum difference between intervention and comparison districts considering neonatal mortality as the main outcome of the MaMoni MNCSP evaluation study. The neonatal mortality rate was 38 per 1,000 life birth (2) and during the sample size calculation; we assumed a 25% reduction of neonatal mortality as per the intervention effect. Considering 2.5:1 intervention to comparison samples size ratio, 80% power, 5% level of significance, 1.5 design effect, and 5% non-response, the calculated sample size was 16,654 in total (11,896 in intervention districts and 4,758 in comparison districts). Secondarily, we also calculated the sample size to estimate the district level coverage of public health facility delivery. Considering 14.3% of public facility delivery prevalence (2), 2.5% absolute precision, 5% non-response and 1.5 design effect, the calculated sample size for each district was ≅1200. So, the total sample size for the 14 evaluation districts was 16,800.
We followed a two-stage stratified cluster sampling process for selecting 1,200 samples from each district. We selected 120 clusters per district and each cluster needed to comprise 10 samples (RDW). Considering the average household size 4.4 and crude birth rate of 21.0 per 1,000 population per year (2), we needed to list at least 120 households to attain ∼10 samples. We conducted the village level clustering and followed the Probability proportional to size (PPS) sampling for the selection of cluster/village within each district. Considering the time and cost involved in a complete listing of households of villages, the project decided not to do a complete listing of all households in each selected village. Alternatively, we selected a section of a village with 120 households. Therefore, we needed a starting point to start listing 120 households for each cluster within the selected village. We used the eligible couple registers maintained by the Family Welfare Assistants (FWA) to randomly select the starting household (index household) to determine starting household. From that index household, we continued till we reach 120 households to complete one cluster. From each cluster we expected to find 10 RDW samples; however, if there were more RDWs we interviewed all.
A total of 18,711 RDW having at least one birth outcome (abortion/stillbirth/live birth) in the past 15 months were interviewed as the study population in the survey. For the analysis, 1,460 women were excluded who experienced an abortion or a stillbirth and included 17,251 RDW with live birth as the study subject. If a woman had twin births, then the last child’s information on neonatal complications and care-seeking behavior was collected. Figure 1 shows the study participant selection for the analysis of this paper.
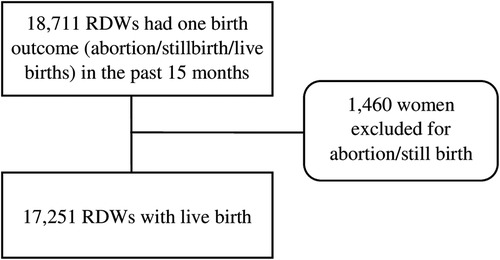
Figure 1. Selection of the sample for the analysis.
Data collection and quality control
The data collection instrument was adapted from the Bangladesh Demographic and Health Survey (BDHS) questionnaire (2, 3). The study investigators pre-tested the adapted questionnaire before data collection. We have prepared the tools in both English and Bangla. However, all interviews were conducted in the Bangla language only. The interview questionnaire included information on socio-demographic characteristics of the households, women’s background characteristics, childbirth history, health service-related information, maternal health care practices, child’s experience of complications, and care-seeking behaviors for sick neonates. We recruited data collectors and supervisors who had extensive experience in survey data collection and most of them had an undergraduate degree in social science. The data collection team comprised 2 field research officers (FRO), 7 field research supervisors (FRS), and 56 data collectors (DC). Each small data collection team consisted of 1 FRS and 8 DC, deployed for the data collection of 2 districts. The FROs supervised all small teams by visiting the team sequentially. All data collectors and supervisors received training on the data collection tools before the start of data collection. Data collection was carried out from April to September 2019. Data was collected on electronic devices, with built-in skips and immediate identification of erroneous entry was built in to improve data quality at the time of entry. FRO and FRS accompanied the DC during data collection. Supervisors organized regular team meetings for supervisory feedback, data rechecking and discussing data collection issues. A quality control (QC) team comprised of interviewers and field-based supervisors monitored and ensured data integrity by re-interviewing and matching with original data. The QC team re-interviewed approximately 3% of the total interviews.
Hypothesized conceptual/theoretical model
Our hypothesized inter-relationship among predictors and main outcome variables was built based on an extensive literature review and the plausibility of inter-relationships (Figure 2). Lines indicate the relationships and direction of relationships between the variables. The lack of a line implies no hypothesized relationship between the variables (34). The variables identified as predictors of care-seeking behaviors for neonatal danger signs were placed into five groups/domains: (1) maternal background characteristics, (2) maternal health care utilization factors, (3) child-related factors, (4) health service-related factors and (5) knowledge on neonatal danger signs. The hypothesized predictors of each domain and scientific evidence used to construct the theoretical model are included in the Supplementary Information S1.
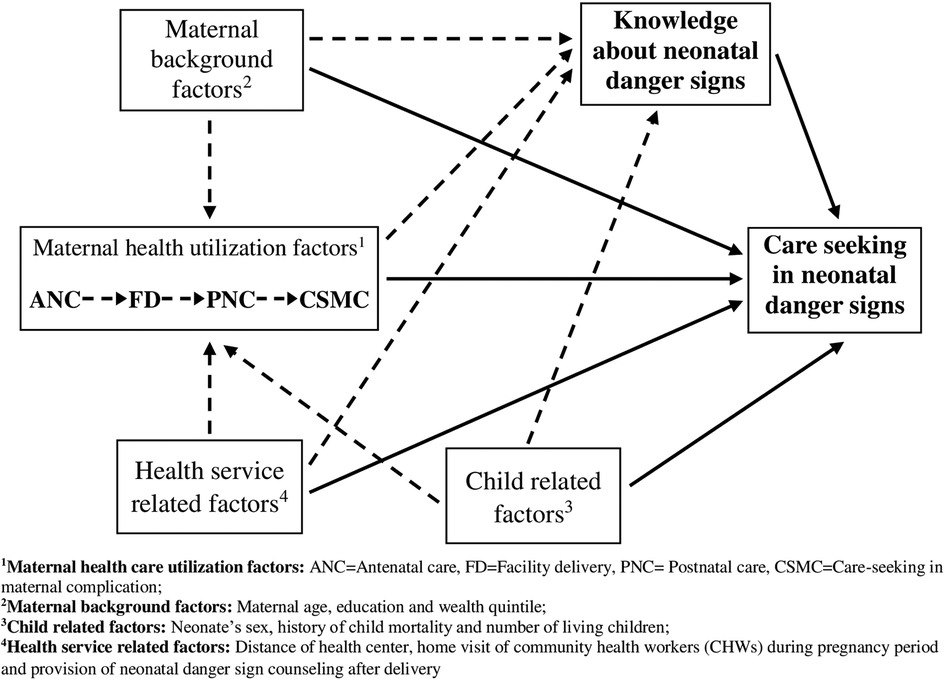
Figure 2. Hypothetical inter-relationship of different factors associated with care-seeking for neonatal danger signs.
Relationships between factors and the main outcome variable are characterized as either direct or indirect relationships. A solid line indicates a direct relationship between the predictor and care-seeking behavior. Whereas, an indirect relationship, that is the mediated relationship through a second predictor variable (called a mediator variable), is represented by the dotted line.
The following Figure 3 is demonstrating the hypothesized direct and indirect effects through mediated pathways for the household wealth and ANC utilization variables. As with Figure 2, the solid represents the direct effect and the dotted arrows show the indirect effects through the mediators.
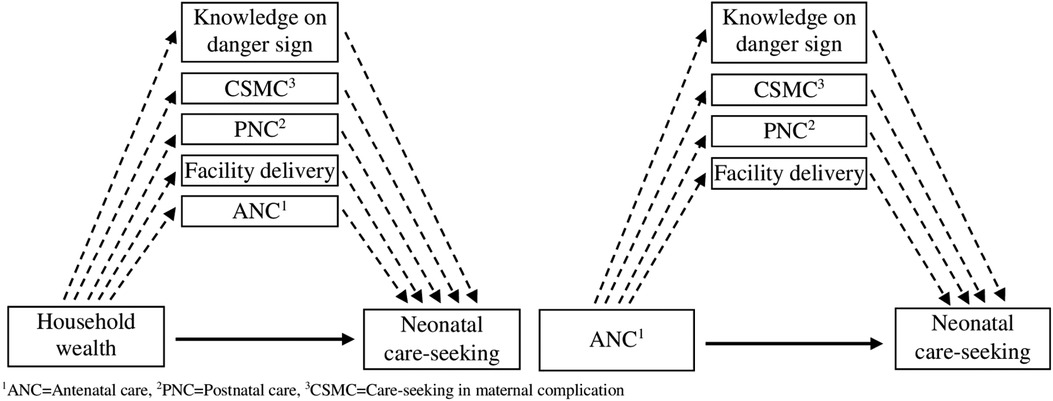
Figure 3. Direct and indirect effect pathway from household wealth and ANC to neonatal care-seeking.
Study variables
Endogenous variables
In the structural equation model, some variables could be simultaneously used as the independent and dependent variables or only the dependent variable. These variables are called endogenous variables. In our GSEM model, six simultaneous multivariable equations of six endogenous/dependent variables were used. The six interrelated endogenous variables were care-seeking for sick neonates from qualified providers, woman’s knowledge of neonatal danger signs, care-seeking for last maternal complication from qualified providers, PNC from qualified providers, facility delivery, and attendance of four or more ANC visits from qualified providers. Medical doctors, nurses, midwives, paramedics, family welfare visitors, medical assistants, sub-assistant community medical officers, and community skilled birth attendants were considered qualified providers (2, 3). Maternal complications were defined as any severe headaches with blurry vision, convulsions, high blood pressure, excessive vaginal bleeding, prolonged labor, body parts except the head coming out first, placenta remaining inside, foul-smelling discharge with high fever, and oedema during pregnancy/delivery/after the delivery period. Knowledge of neonatal danger signs was measured as the number of danger signs for which care should be sought. The interview question consisted of 22 danger sign options, which included difficulty or fast breathing, pneumonia, cold/cough, low temperature, high temperature, yellow skin/eye, poor sucking or feeding, discharge from the umbilical cord, skin lesions/blisters, red or swollen eyes with pus, skin rash, measles, convulsions/spasms/rigidity, lethargy/unconsciousness, baby doesn’t cry, doesn’t pass urine, doesn’t pass stool, continuous vomiting, distended abdomen, difficult to wake, diarrhea, and chest in-drawing. Interviewers did not read out the danger signs options while asking this question. For the following question, interviewers read out all the above mentioned danger signs and asked the women whether the child experienced any of these danger signs. Then the subsequent care-seeking behavior was asked. As endogenous variable neonatal danger sign knowledge was used as a continuous variable. All the other endogenous variables were binomial, categorized as yes or no.
Exogenous variables
All the variables used only as independent variables in the structural model are called exogenous variables. The exogenous variables included in the model were maternal age, education, wealth quintile, the total number of live children, history of child death, sex of newborn, distance to the nearest health facility, facility delivery, home visit by a community health worker (CHW) during the pregnancy period, and receipt of any counseling on neonatal danger signs after delivery. We categorized the distance to the nearest health facility into two categories (<5 km and 5 km or more) and operationally defined “<5 km” as the near distance and “5 km and more” as the long distance (2, 3). For the construction of the household wealth quintile, we used household assets, construction materials of household (roof, walls, and floor), source of drinking water, toilet type, number of rooms in the household, ownership of homestead and agricultural land, ownership of domestic animals (cattle, goat, and chicken) and type of fuel used for cooking. For the exogenous variable on women’s knowledge of neonatal danger signs, it was categorized into three categories (0, 1–4, and 5+). We operationally defined the danger sign knowledge of less than 5 as low knowledge of newborn danger signs (86). Consistent with other similar literature, the standard category of other exogenous variables was used in the structured equation model (9, 21, 23, 26, 40–42).
Data analysis
First, we did a descriptive summary of all maternal background characteristics, child-related factors, health service-related factors, and all maternal and child health utilization factors. The descriptive analysis was also done among healthy neonates and sick neonates. Then, we used GSEM in the subpopulation of sick neonates (N = 8765) to estimate the inter-relationships of the predictor variables and newborn care-seeking. In our GSEM model, we used the Bernoulli family and logit link function for binary endogenous variables (4 + ANC from qualified providers, facility delivery, PNC from qualified providers, care-seeking of maternal complication, and care-seeking of sick neonates) and gaussian family and identity link function for the continuous endogenous variable (knowledge on neonatal danger signs) (36). Additionally, the robust standard error was considered as mitigation of the multivariate normality (MVN) assumption (37). The indirect (mediated) effect of each indirect pathway of each mediator was calculated with multiplicated coefficients. The total indirect effect of the variable was estimated by the sum of multiplicated coefficients of all mediated pathways. The total effect of each indicator was calculated as a sum of the direct and total indirect effects. These indirect, direct, and total effects were obtained using the “nlcom” post-estimation command after the GSEM model. All the indirect, direct, and total effects were estimated and reported in terms of Log Odds (LOD), which has the linear additive property. Using LOD calculation of mediating proportion and cross-comparison of effect can be made. The mediation proportion was calculated by dividing the indirect over the total effect (38). Due to the comparability of effects across the predictors, the average relative effect was calculated for the multi-categorical independent variable (39). As a supplementary analysis, we also conducted the distribution of very severe neonatal complications according to neonate’s sex (Supplementary Table S1) and the care-seeking distribution of qualified and unqualified providers according to reported very severe complications (Supplementary Table S2). All data analysis was conducted in STATA, version 14.0.
Ethical consideration
Ethical approval was granted by the Ethical Review Committee of Save the Children USA and the Institutional Review Board (IRB) of icddr,b (Protocol number: PR#18099). Informed written consent was obtained from the study participants after explaining the purpose of the data collection, methods and procedure, use of data, risks, benefits, principle of no compensation, measures for privacy and confidentiality, their voluntary participation, and right to withdraw from the study at any time without showing any cause. For mothers below 18 years, we also took informed written consent from a legal guardian or next of kin.
Results
Description of study participants
The majority of mothers were between 20 and 34 years of age (76.9%) and 15.2% of mothers were less than 20 years. About 7.3% of mothers had no education, 12.5% stopped school before completing primary education, and only 21.3% completed secondary or higher levels of study. Overall, 34.7% of mothers reported that this was their first child and 10% experienced a child death in the past.
Overall, less than one-third (27.3%) of mothers received four or more ANC visits from qualified providers during their last pregnancy, around half (52.2%) gave birth in a health facility, 43.4% received PNC from qualified providers, and 65.0% sought care from qualified providers during their most recent maternal complication (N = 4713). Mothers’ knowledge of neonatal danger signs was low. Out of 22 neonatal danger signs, 3.3% of mothers of sick neonates had no knowledge of any neonatal danger sign, 76.4% knew 1–4 danger signs and only 20.3% of mothers knew 5 or more danger signs (Table 1).
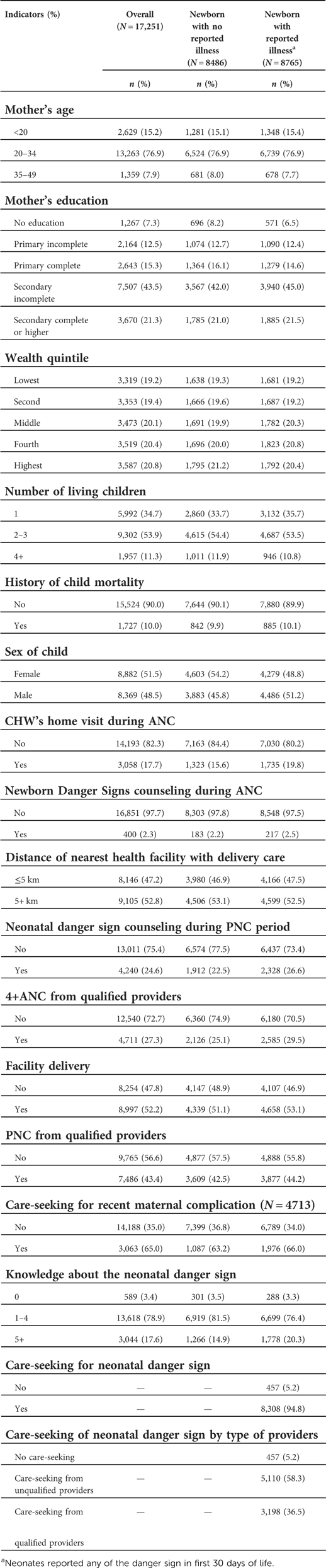
Table 1. Distribution of overall background characteristics of the respondents, and disaggregated by the healthy and sick neonates.
Among all mothers, 8,765 mothers (50.8%) reported that their newborns experienced at least one danger sign in the first month of life. Among the mothers of those sick neonates, almost all (94.4%) sought care from any type of provider, however, only about one-third (36.5%) sought care from a qualified provider (Table 1). Among severe neonatal danger signs, care-seeking from qualified providers was high for difficult or fast breathing (45.4%), chest in-drawing (50.0%), and fever (43.8%) (Supplementary Table S2).
Identification of direct and indirect predictors and effect pathways on newborn care-seeking
Table 2 details the inter-relationship among maternal health utilization indicators, neonatal danger sign knowledge, maternal background characteristics, child/neonate-related factors, and health service-related factors to explain neonatal care-seeking behavior. In the supplementary materials, we have included a table (Supplementary Table S3) that summarizes the significant inter-relationships of the GSEM model (Table 2), i.e., the significant direct and indirect effect pathway and the effect measures of predictors and mediators on the main outcome variable.
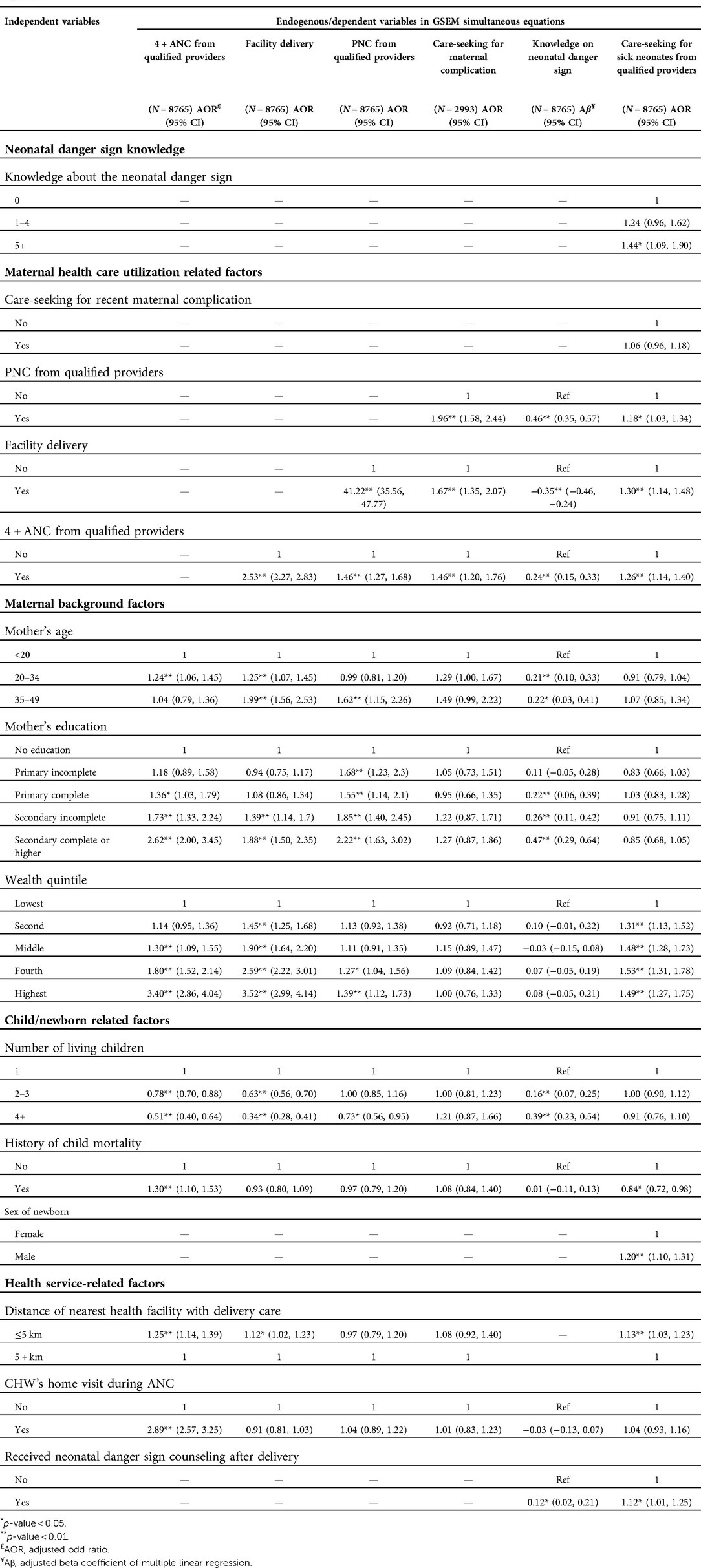
Table 2. Analysis of interrelationship among the maternal health utilization factors, maternal background factors, child/neonatal factors, health service factors, neonatal danger sign knowledge and the care-seeking for sick neonates as per hypothetical inter-relationship framework (figure 2) using generalized structural equation modeling (GSEM).
Neonatal care-seeking from a qualified provider was associated with maternal danger sign knowledge. The adjusted odd of neonatal care-seeking behavior was higher among mothers with knowledge of 5 or more neonatal danger signs compared to mothers with no knowledge of neonatal danger signs (AOR: 1.44, 95% CI: 1.09, 1.90). Neonatal care-seeking behavior was not directly associated with maternal care-seeking behavior during complications (AOR: 1.06, 95% CI: 0.96, 1.18).
Three maternal health care utilization indicators (PNC from a qualified provider, facility delivery, and 4 + ANC from a qualified provider) were both directly and indirectly associated with neonatal care-seeking behavior. Mothers who received a PNC visit from a qualified provider were slightly more likely to seek care when their newborn exhibited danger signs (AOR: 1.18, 95% CI: 1.03, 1.34). In addition, maternal PNC also mediated the newborn care-seeking indirectly by increasing the knowledge of neonatal danger signs greatly (Aβ: 0.46, 95% CI: 0.35, 0.57). Among the maternal health utilization factors, health facility delivery directly increased the adjusted odds of care-seeking for neonatal illness (AOR: 1.30, 95% CI: 1.14, 1.48) and indirectly mediated the care-seeking by increasing the odds of receiving a maternal PNC visit (AOR: 41.22, 95% CI: 35.56, 47.77). On the other hand, attending 4 + ANC visits during pregnancy directly increased the odds of neonatal care-seeking behavior of mothers (AOR: 1.26, 95% CI: 1.14, 1.40) and indirectly increased the odds of neonatal care-seeking through increasing the likelihood of receiving a maternal PNC visit (AOR: 1.46, 95% CI: 1.27, 1.68), facility delivery (AOR: 2.53, 95% CI: 2.27, 2.83) and knowledge of neonatal danger signs (Aβ: 0.24, 95% CI: 0.15, 0.33).
Among the maternal background characteristics, only household wealth was directly associated with neonatal care-seeking. The odds of care-seeking for newborn illness increased with household wealth, mothers from households in the higher wealth quintiles were 1.3–1.5 times more likely to seek care than mothers from households in the lowest wealth quintile. Additionally, the wealth quintile indirectly mediated the neonatal care-seeking by increasing the odds of receiving ANC (AOR ranged: 1.30–3.40), facility delivery (AOR ranged: 1.45–3.52), and PNC (AOR ranged: 1.27–1.39). On the other hand, maternal education only indirectly increased the odds of neonatal care-seeking through increasing the knowledge of neonatal danger signs (Aβ ranged: 0.22–0.47), maternal PNC (AOR ranged: 1.68–2.22), facility delivery (AOR ranged: 1.39–1.88) and four or more ANC (AOR ranged: 1.36–2.62) in higher educated groups. Likewise, maternal age also was not associated with neonatal care-seeking behavior directly, however, it significantly increased the neonatal danger sign knowledge consistently (Aβ ranged: 0.22–0.47).
Among the child-related factors, neonatal care-seeking was higher for male children compared to female children (AOR: 1.20, 95% CI: 1.10, 1.31). This could be due to the higher percentage of male children who experienced severe danger signs (54.4%, p = 0.001) compared to female children (50.8%); and no difference was seen in qualified care-seeking (p = 0.075) during those severe danger signs (Supplementary Table S1). The odds of care-seeking were lower among mothers who had a history of child death (AOR: 0.84, 95% CI: 0.72, 0.97). Having more children significantly decreased the odds of ANC, facility delivery, and PNC, but increased the odds of knowledge of neonatal danger signs.
Among health service indicators, a shorter distance to the nearest health facility (≤5 km) not only directly increased the likelihood of neonatal care-seeking behavior (AOR: 1.13, 95% CI: 1.03, 1.23) but also indirectly increased the odds of neonatal care-seeking by increasing the odds of ANC (AOR: 1.25, 95% CI: 1.14, 1.39) and facility delivery (AOR: 1.12, 95% CI: 1.02, 1.23). Furthermore, receipt of counseling on neonatal danger signs not only directly increased the chance of neonatal care-seeking (AOR: 1.12, 95% CI: 1.01, 1.25) but also indirectly increased neonatal care-seeking by increasing knowledge of neonatal danger signs (Aβ: 0.12, 95% CI: 0.02, 0.21). Having received a CHW home visit during ANC did not impact care-seeking (AOR: 1.04, 95% CI: 0.93, 1.16), though it might have some positive indirect impact on care-seeking by increasing the odds a woman received ANC (AOR: 2.89, 95% CI: 2.57, 3.25).
Estimating the direct, indirect and total effect of predictor variables on newborn care-seeking
Table 3 shows the decomposition of direct, indirect, and summative total effect (in terms of Log Odds) of the significant inter-related predictors on neonatal care-seeking identified in the above GSEM model (Table 2).
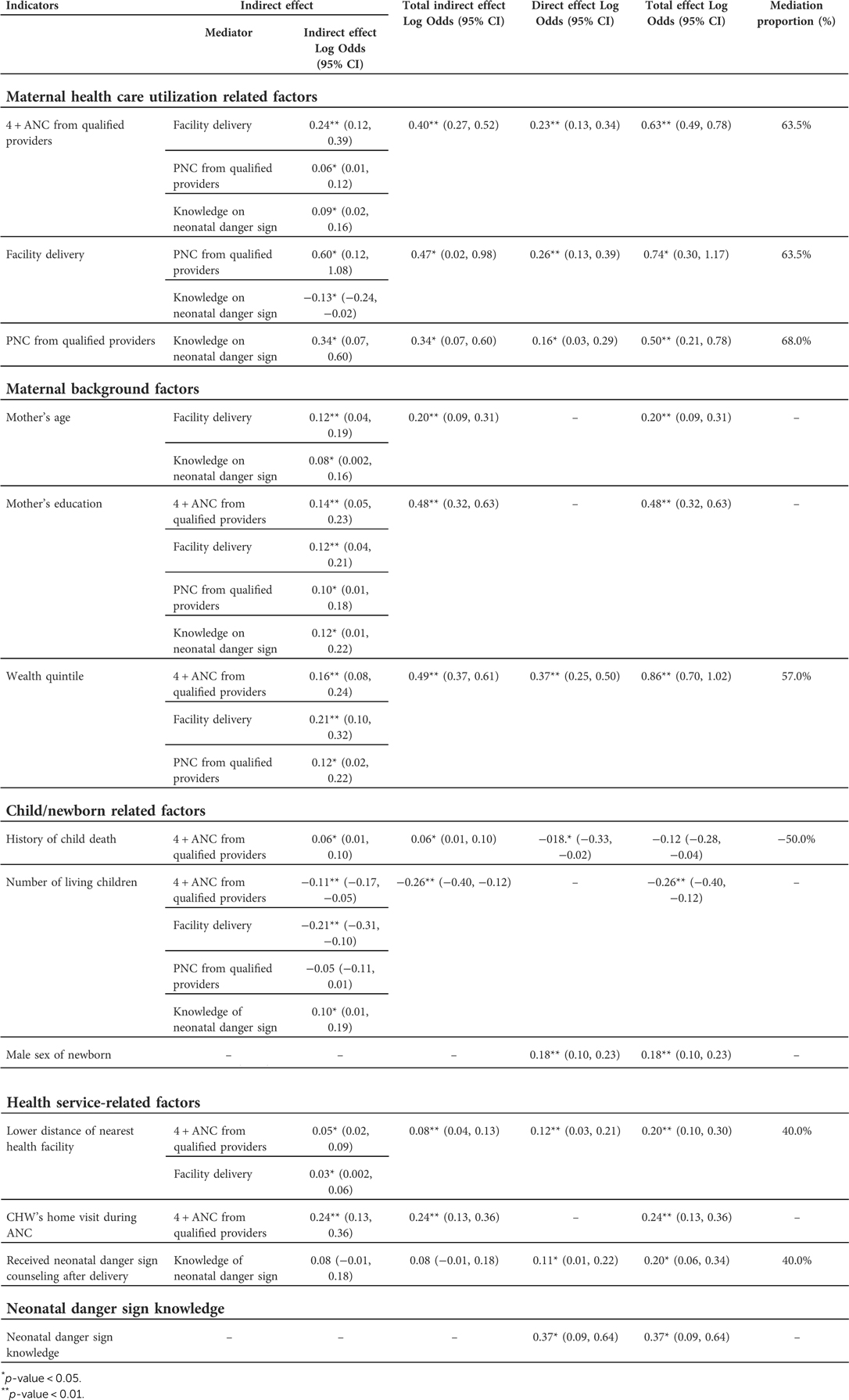
Table 3. Indirect effect, direct effect, total effect and mediating proportion of predictors on neonatal care-seeking (mediation analysis result).
Among the maternal health care indicators, ANC, facility delivery, and PNC had a direct effect on neonatal care-seeking [ANC::Log Odds (LOD): 0.23, 95% CI: 0.13, 0.34; Facility delivery::LOD: 0.26, 95% CI: 0.13, 0.39; PNC::LOD: 0.16, 95% CI: 0.03, 0.29]. Similarly, ANC, facility delivery and PNC also indirectly increased neonatal care-seeking [ANC::Log Odds (LOD): 0.23, 95% CI: 0.13, 0.34; Facility delivery::LOD: 0.26, 95% CI: 0.13, 0.39; PNC::LOD: 0.16, 95% CI: 0.03, 0.29]. The proportions of indirect effects of ANC, facility delivery and PNC were higher than the direct effect (Mediation proportion range: 63.5%–68.0%). ANC had 3 mediating pathways, and among those, facility delivery was the most proximate to the ANC and mediated the highest indirect effect (LOD: 0.24). Similarly, facility delivery had 2 mediating pathways and the highest indirect effect of facility delivery was mediated through PNC (LOD: 0.60). Finally, all of the indirect effects of PNC were mediated through the women’s knowledge of neonatal danger signs (LOD: 0.34). Maternal health utilization factors (ANC, facility delivery, and PNC) had the highest summative total effects (Log Odds (LOD): 1.80) comparing the summative total effect of each maternal background, child/newborn, and health service-related factors.
Among the maternal background factors, household wealth had both direct (LOD: 0.37, 95% CI: 0.25, 0.50) and indirect effects (LOD: 0.49, 95% CI: 0.37, 0.61). This indirect effect was also the highest among all indirect effects and mediated through ANC, facility delivery, and PNC. Household wealth showed the highest total effect (LOD: 0.86, 95% CI: 0.70, 1.02) among all other predictors of neonatal care-seeking. On the other hand, maternal education did not show any direct effect, though it showed the second highest indirect effect among all other predictors of neonatal care-seeking (LOD: 0.48, 95% CI: 0.32, 0.63).
Among the child-related factors, the likelihood of neonatal care-seeking was higher among the male children (LOD: 0.18, 95% CI: 0.10, 0.23), while care-seeking was less among mothers who had a history of child death (LOD: −0.12, 95% CI: −0.28, −0.04). Similarly, neonatal care-seeking was lower among the mothers with more children (LOD: −0.26, 95% CI: −0.40, −0.12).
Among the health service-related indicators, receipt of a CHW visit during pregnancy indirectly increased neonatal care-seeking (LOD: 0.24, 95% CI: 0.13, 0.36). Following the CHW visit, distance to the nearest health facility and receiving counseling on neonatal danger signs after delivery each increased the total log odds of neonatal care-seeking by 0.20 times (95% CI: 0.10, 0.30 and 0.06, 0.34 respectively).
On the other hand, as the most proximal predictor, women’s knowledge of neonatal danger signs only directly increased the log odds of neonatal care-seeking (LOD: 0.37, 95% CI: 0.09, 0.64). It was also the significant mediating channel for most other variables of the conceptual framework.
Discussion
This study found a high prevalence (one of every two neonates) of neonatal danger signs in the first month after birth, which was consistent with the findings of other studies conducted in Bangladesh (9, 26). Although almost all mothers of infants with danger signs sought care, only one-third sought care from a qualified health provider, which was consistent with a recent study in Bangladesh (23). Two-thirds of mothers sought care from untrained providers, which include village doctors, homeopathic practitioners, and local drug stores. In Bangladesh, village doctors are the most frequent choice due to easy access, and because their services are relatively cheap and culturally acceptable (21, 23, 26, 40, 41). In addition, parents believe that homeopathic medicine is mild and has a gentle effect, is easy to administer, and has no side effects, and thus, is considered more suitable for neonates (26, 42). Training of unqualified providers on timely referral to health facilities could be considered to facilitate the appropriate diagnosis and treatment of sick neonates (26).
Among the maternal health utilization factors, ANC, facility delivery, and PNC from qualified providers directly increased neonatal care-seeking from a qualified provider, which was similar to other studies (23, 24, 43, 44). Previous visits to qualified providers increase not only the trust, but also awareness about the availability of newborn care services, and the importance of care-seeking from trained health personnel during an illness episode (23, 26, 45). On the other hand, the indirect effects of ANC, facility delivery and PNC were larger than the direct effect. In conventional determinant analysis, only the direct effects are calculated, which underestimates the overall total effect of a predictor variable on the outcome variable. Therefore, in addition to the direct effect, the greater indirect effect implies the further importance of these factors as the determinants of neonatal care-seeking.
In summary, the highest summative effect of maternal health factors (ANC, facility delivery, and PNC) on newborn care-seeking over other factors domains suggests that ensuring mothers’ use of services along the continuum from pregnancy through the postnatal period should be the key programmatic focus of maternal and child health care interventions. For improving the maternal care continuum, some integrated community and health facility-based interventions with the deployment of adequate community-based skilled providers with strong monitoring for continuity were found successful in Bangladesh (46, 47) and other countries (48–50). But further scaling up requires addressing some policy-level challenges, such as recognition of community-based intervention, increasing sustainability and retention of community health workers, addressing the shortage of human resources in public health care, ensuring health workers stay at primary level facilities and innovation in public-private partnership (46, 47, 51). For a resource-poor country like Bangladesh, mobile health (mHealth) strategies have shown promise to improve the timely maternal care continuum (52–54). The national health information management system (HMIS) could be leveraged by integrating a low-cost mHealth innovation within it. Studies also identified the quality of care of maternal health services as an important determinant of the utilization of an adequate number of ANC, facility delivery, and PNC from skilled providers (51, 55–57). Therefore, the quality of maternal care also needs to be prioritized as part of health system strengthening efforts.
Household economic status had the highest total effect on newborn care-seeking, with an almost equal amount of direct and indirect effects; and all indirect effects were mediated through ANC, facility delivery, and PNC. Household income is an enabling factor for care-seeking; and it is obvious that the treatment, medicine, transportation, and opportunity cost for care-seeking are key barriers for poorer households (58–60). In many settings including Bangladesh, demand-side financing (DSF) schemes, such as conditional cash transfers or vouchers; and expansion of services in low-coverage areas for the poorer households have been reported to be effective to reduce inequities for all socioeconomic groups in maternal and child healthcare utilization (61–64). On the other hand, maternal education did not show any direct effect on neonatal care-seeking, which was similar to other study findings (24, 26). However, maternal education did indirectly show a substantial effect on neonatal care-seeking through ANC, facility delivery, PNC, and the mother’s knowledge of newborn danger signs. The total indirect effect size of maternal education was large enough to show that maternal education is an important positive factor for improving neonatal care-seeking.
Our study results showed higher care-seeking practices for male newborns compared to females. However, this higher likelihood of care-seeking was explained by the higher number of severe complications among the male neonates, but equal care-seeking proportion during those complications (Supplementary Table S1). Previous studies from Bangladesh have shown a significant sex differential in neonatal care-seeking (21, 24, 26, 65, 66); while our study suggests that there is no apparent gender bias in neonatal care-seeking.
Among the health service-related factors, distance to the nearest health facility was directly and indirectly associated with neonatal care-seeking from qualified providers, which is a similar finding to other studies conducted in Bangladesh (24, 67). Long distance to the nearest health facility is a major barrier to accessing health care services (68–71). The government’s standard operating procedure for sick newborns requires referring to Upazila Health Complex (UHC) or District Hospital (DH) (72). At the sub-district level, there is only one UHC (73) and mothers may refuse referral for various reasons including distance to the referral facility, poor roads, or lack of transportation. However, sick newborns with suspected bacterial infections who can’t be referred for any reason need to be treated with antibiotics at a primary (Union) level facility (74). The government should encourage and improve local providers’ adherence to guidelines for antibiotic treatment for referral-refused mothers (74). Among other health service factors, counseling on neonatal danger signs after delivery, however, did demonstrate a positive effect in increasing woman’s knowledge of neonatal danger signs and subsequently increasing the likelihood of care-seeking from qualified providers for newborn illness (24).
In our conceptual model, neonatal danger sign knowledge was the most proximal factor to neonatal care-seeking; having only a direct effect on care-seeking (75–78) and serving as a mediating channel for most factors to affect neonatal care-seeking for illness episodes. Our study results showed low knowledge levels among women about danger signs. The care-seeking from qualified providers was high if mothers perceived the danger signs as severe (49.0%). However, for actual medically identified severe neonatal danger signs (79–83), care-seeking was low (35.6%) (Supplementary Table S2), which implied the wrong judgment about the severity of danger signs (84). This evidence deems the importance of raising maternal awareness about newborn danger signs, most importantly, raising awareness regarding the severity and subsequent qualified care-seeking options. Counseling and health education should be strengthened at the available contact points during the antenatal, delivery, and postnatal periods at the facility and in the community (75, 78).
Strengths and limitations
To our knowledge this is the first study that assessed the direct, indirect, and total effect of predictor variables in explaining neonatal care-seeking for neonatal illness/danger signs through GSEM and mediation analysis, using a population-based survey with large sample size. However, our study has some limitations. The data used in our study was cross-sectional and therefore the analysis can’t confirm the direction of causality between variables. Additionally, SEM/GSEM analysis is based on a hypothetical model with some simultaneous multivariable regression models. Perfect model identification for each simultaneous regression model may not possible due to variables’ availability given the nature of the study and dataset, which may lead to omitted variable bias (37, 85).
Conclusions
Unqualified village practitioners are the first contacts for most of the mothers of sick neonates. Therefore, training the informal providers on the timely referral of sick neonates to health facilities is important. The inter-relationship and highest summative effect of ANC, facility delivery, and PNC on newborn care-seeking suggested that ensuring the maternal care continuum altogether should be the key programmatic focus of maternal and child health care interventions to improve sick newborn care-seeking. Targeted intervention for poorer households and increasing the community health worker’s home visits are also required to improve neonatal care-seeking. The effectiveness of danger sign counseling and higher maternal knowledge deemed the importance of danger sign counseling by the health care providers at the available contact points during the antenatal, delivery, and postnatal period at the facility and in the community. In summary, integrated community and health facility-based strategy combined with the innovation of health system strengthening should be the foundation of maternal and newborn health care utilization and saving newborn lives.
Data availability statement
The datasets presented in this article are not readily available because Due to ethical restrictions related to protecting study participants’ privacy and confidentiality, data access is restricted by the Ethical Review Committee of icddr,b. According to the icddr,b data policy ( interested parties may contact Ms. Armana Ahmed ([email protected]) with further inquiries related to data access. Requests to access the datasets should be directed to Ms. Armana Ahmed ([email protected]).
Ethics statement
The studies involving human participants were reviewed and approved by Ethical Review Committee of Save the Children USA and Institutional Review Board (IRB) of International Centre for Diarrhoeal Disease Research, Bangladesh (Protocol number: PR#18099). The patients/participants provided their written informed consent to participate in this study.
Author contributions
SB, BB, SZ, UM and SA: contributed to the design of the MaMoni MNCSP project. SP: supervised the data collection. RA and SB: conceptualized the data analysis and prepared concept version of the manuscript under the guidance of SA. RA did the data analysis, wrote the first draft and addressed the comments of co-authors. BB, NA, SH, JJ, LG, SP SZ, SR, MR, UM, SA: critically reviewed the manuscript. SB, SH, JJ, LG: edited the paper. All authors contributed to the article and approved the submitted version.
Acknowledgments
United States Agency for International Development (USAID) funded the MaMoni Maternal and Newborn Care Strengthening Project (MNCSP). With gratitude, we acknowledge USAID’s commitment towards the implementation research in Bangladesh. icddr,b is always grateful to the governments of Bangladesh, UK, Sweden and Canada for their unrestricted/core support. We are also thankful to our data collectors, supervisors and data management team for their valuable contribution in this study. Before anything else, we are thankful to our study participants and their families for their kind cooperation during data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at:
References
1. United Nations Children’s Fund (UNICEF), World Health Organization (WHO), World Bank Group and United Nations Population Division. Levels and trends in child mortality: Report 2019. United Nations Children’s Fund (2019).
2. National Institute of Population Research and Training (NIPORT) and ICF International. Bangladesh Demographic and health survey 2017–18. NIPORT, and ICF International (2020).
3. National Institute of Population Research and Training (NIPORT), Mitra and Associates and ICF International. Bangladesh demographic and health survey 2014. NIPORT, Mitra and Associates and ICF International (2016).
4. Halim A, Dewez JE, Biswas A, Rahman F, White S, van den Broek N. When, where, and why are babies dying? Neonatal death surveillance and review in Bangladesh. PloS one. (2016) 11(8):e0159388. doi: 10.1371/journal.pone.0159388
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Khatun F, Rasheed S, Moran AC, Alam AM, Shomik MS, Sultana M, et al. Causes of neonatal and maternal deaths in Dhaka slums: implications for service delivery. BMC Public Health. (2012) 12(1):1–9. doi: 10.1186/1471-2458-12-84
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Chowdhury HR, Thompson S, Ali M, Alam N, Yunus M, Streatfield PK. Causes of neonatal deaths in a rural subdistrict of Bangladesh: implications for intervention. J Health Popul Nutr. (2010) 28(4):375. doi: 10.3329/jhpn.v28i4.6044
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Fottrell E, Osrin D, Alcock G, Azad K, Bapat U, Beard J, et al. Cause-specific neonatal mortality: analysis of 3772 neonatal deaths in Nepal, Bangladesh, Malawi and India. Arch Dis Child Fetal Neonatal Ed. (2015) 100(5):F439–F47. doi: 10.1136/archdischild-2014-307636
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Arifeen SE, Hoque DE, Akter T, Rahman M, Hoque ME, Begum K, et al. Effect of the integrated management of childhood illness strategy on childhood mortality and nutrition in a rural area in Bangladesh: a cluster randomised trial. Lancet. (2009) 374(9687):393–403. doi: 10.1016/S0140-6736(09)60828-X
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Bari S, Mannan I, Rahman MA, Darmstadt GL, Seraji MHR, Baqui AH, et al. Trends in use of referral hospital services for care of sick newborns in a community-based intervention in tangail district, Bangladesh. J Health Popul Nutr. (2006) 24(4):519. doi: 10.3329/JHPN.V24I4.704
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Darmstadt GL, Arifeen SE, Choi Y, Bari S, Rahman SM, Mannan I, et al. Household surveillance of severe neonatal illness by community health workers in mirzapur, Bangladesh: coverage and compliance with referral. Health Policy Plan. (2010) 25(2):112–24. doi: 10.1093/heapol/czp048
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Ronsmans C, Chowdhury ME, Koblinsky M, Ahmed A. Care seeking at time of childbirth, and maternal and perinatal mortality in matlab, Bangladesh. Bull W H O. (2010) 88(4):289–96. doi: 10.2471/BLT.09.069385
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Azad K, Barnett S, Banerjee B, Shaha S, Khan K, Rego AR, et al. Effect of scaling up women’s Groups on birth outcomes in three rural districts in Bangladesh: a cluster-randomised controlled trial. Lancet. (2010) 375(9721):1193–202. doi: 10.1016/S0140-6736(10)60142-0
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Baqui AH, El-Arifeen S, Darmstadt GL, Ahmed S, Williams EK, Seraji HR, et al. Effect of community-based newborn-care intervention package implemented through two service-delivery strategies in sylhet district, Bangladesh: a cluster-randomised controlled trial. Lancet. (2008) 371(9628):1936–44. doi: 10.1016/S0140-6736(08)60835-1
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Herbert HK, Lee AC, Chandran A, Rudan I, Baqui AH. Care seeking for neonatal illness in low-and middle-income countries: a systematic review. PLoS Med. (2012) 9(3):e1001183. doi: 10.1371/journal.pmed.1001183
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Waiswa P, Kallander K, Peterson S, Tomson G, Pariyo GW. Using the three delays model to understand why newborn babies die in eastern Uganda. Trop Med Int Health. (2010) 15(8):964–72. doi: 10.1111/j.1365-3156.2010.02557.x
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Lawn JE, Kerber K, Enweronu-Laryea C, Cousens S. editors. 3.6 Million neonatal deaths—what is progressing and what is not? Seminars in perinatology. Elsevier (2010). doi: 10.1053/j.semperi.2010.09.011
18. Hill Z, Manu A, Tawiah-Agyemang C, Gyan T, Turner K, Weobong B, et al. How did formative research inform the development of a home-based neonatal care intervention in rural Ghana? J Perinatol. (2008) 28(2):S38–45. doi: 10.1038/jp.2008.172
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Syed U, Khadka N, Khan A, Wall S. Care-seeking practices in south Asia: using formative research to design program interventions to save newborn lives. J Perinatol. (2008) 28(2):S9–S13. doi: 10.1038/jp.2008.165
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Tinuade O, Iyabo RA, Durotoye O. Health-care-seeking behaviour for childhood illnesses in a resource-poor setting. J Paediatr Child Health. (2010) 46(5):238–42. doi: 10.1111/j.1440-1754.2009.01677.x
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Chowdhury HR, Thompson SC, Ali M, Alam N, Yunus M, Streatfield PK. Care seeking for fatal illness episodes in neonates: a population-based study in rural Bangladesh. BMC Pediatr. (2011) 11(1):1–8. doi: 10.1186/1471-2431-11-88
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Baqui A, El-Arifeen S. Community-based intervention to reduce neonatal mortality in Bangladesh. PROJAHNMO–I: project for advancing the health of newborns and mothers. Sylhet District, Bangladesh: Johns Hopkins Bloomberg School of Public Health (JHSPH) and International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR, B) (2007).
23. Chowdhury SK, Billah SM, Arifeen SE, Hoque DME. Care-seeking practices for sick neonates: findings from cross-sectional survey in 14 rural sub-districts of Bangladesh. PloS One. (2018) 13(9):e0204902. doi: 10.1371/journal.pone.0204902
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Shah R, Mullany LC, Darmstadt GL, Talukder RR, Rahman SM, Mannan I, et al. Determinants and pattern of care seeking for preterm newborns in a rural Bangladeshi cohort. BMC Health Serv Res. (2014) 14(1):1–12. doi: 10.1186/1472-6963-14-417
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Nonyane BA, Kazmi N, Koffi AK, Begum N, Ahmed S, Baqui AH, et al. Factors associated with delay in care–seeking for fatal neonatal illness in the sylhet district of Bangladesh: results from a verbal and social autopsy study. J Glob Health. (2016) 6(1):320–9. doi: 10.7189/jogh.06.010605
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Witt ST, Meyerand ME. The effects of computational method, data modeling, and TR on effective connectivity results. Brain Imaging Behav. (2009) 3(2):220–31. doi: 10.1007/s11682-009-9064-5
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Lau Y, Htun TP, Lim PI, Ho-Lim S, Klainin-Yobas P. Maternal, infant characteristics, breastfeeding techniques, and initiation: structural equation modeling approaches. PLoS One. (2015) 10(11):e0142861. doi: 10.1371/journal.pone.0142861
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Marsh HW, Lüdtke O, Muthén B, Asparouhov T, Morin AJ, Trautwein U, et al. A new look at the big five factor structure through exploratory structural equation modeling. Psychol Assess. (2010) 22(3):471. doi: 10.1037/a0019227
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Jacobs SR, Weiner BJ, Reeve BB, Hofmann DA, Christian M, Weinberger M. Determining the predictors of innovation implementation in healthcare: a quantitative analysis of implementation effectiveness. BMC Health Serv Res. (2015) 15(1):1–13. doi: 10.1186/s12913-014-0652-8
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Rabe-Hesketh S, Skrondal A, Pickles A. Generalized multilevel structural equation modeling. Psychometrika. (2004) 69(2):167–90. doi: 10.1007/BF02295939
CrossRef Full Text | Google Scholar
32. Mendola P, Mumford SL, Männistö TI, Holston A, Reddy UM, Laughon SK. Controlled direct effects of preeclampsia on neonatal health after accounting for mediation by preterm birth. Epidemiology. (2015) 26(1):17. doi: 10.1097/EDE.0000000000000213
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Liu S-H, Ulbricht CM, Chrysanthopoulou SA, Lapane KL. Implementation and reporting of causal mediation analysis in 2015: a systematic review in epidemiological studies. BMC Res Notes. (2016) 9(1):1–21. doi: 10.1186/s13104-015-1837-x
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Violato C, Hecker KG. How to use structural equation modeling in medical education research: a brief guide. Teach Learn Med. (2007) 19(4):362–71. doi: 10.1080/10401330701542685
PubMed Abstract | CrossRef Full Text | Google Scholar
35. icddrb&SaveTheChildren. Monitoring the progress and evaluating the impact of quality maternal and newborn care services in MaMoni MNCSP programme districts in Bangladesh: Study Protocol. (Unpublished) (2018).
36. StataCorp. Structural equation modeling reference manual. Release 14. StataCorp LP (2015).
37. Tomarken AJ, Waller NG. Structural equation modeling: strengths, limitations, and misconceptions. Annu Rev Clin Psychol. (2005) 1:31–65. doi: 10.1146/annurev.clinpsy.1.102803.144239
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Ditlevsen S, Christensen U, Lynch J, Damsgaard MT, Keiding N. The mediation proportion: a structural equation approach for estimating the proportion of exposure effect on outcome explained by an intermediate variable. Epidemiology. (2005) 16(1):114–20. doi: 10.1097/01.ede.0000147107.76079.07
PubMed Abstract | CrossRef Full Text | Google Scholar
40. Arifeen S E, Baqui AH, Victora CG, Black RE, Bryce J, Hoque D, et al. Sex and socioeconomic differentials in child health in rural Bangladesh: findings from a baseline survey for evaluating integrated management of childhood illness. J Health Popul Nutr. (2008) 26(1):22.18637525
PubMed Abstract | Google Scholar
43. Taffa N, Chepngeno G. Determinants of health care seeking for childhood illnesses in Nairobi slums. Trop Med Int Health. (2005) 10(3):240–5. doi: 10.1111/j.1365-3156.2004.01381.x
PubMed Abstract | CrossRef Full Text | Google Scholar
44. Sreeramareddy CT, Shankar RP, Sreekumaran BV, Subba SH, Joshi HS, Ramachandran U. Care seeking behaviour for childhood illness-a questionnaire survey in western Nepal. BMC Int Health Hum Rights. (2006) 6(1):1–10. doi: 10.1186/1472-698X-6-7
PubMed Abstract | CrossRef Full Text | Google Scholar
45. Pervin J, Moran A, Rahman M, Razzaque A, Sibley L, Streatfield PK, et al. Association of antenatal care with facility delivery and perinatal survival–a population-based study in Bangladesh. BMC Pregnancy Childbirth. (2012) 12(1):1–12. doi: 10.1186/1471-2393-12-111
PubMed Abstract | CrossRef Full Text | Google Scholar
46. Huq NL, Ahmed A, Haque NA, Hossaine M, Uddin J, Ahmed F, et al. Effect of an integrated maternal health intervention on skilled provider’s Care for maternal health in remote rural areas of Bangladesh: a pre and post study. BMC Pregnancy Childbirth. (2015) 15(1):1–15. doi: 10.1186/s12884-015-0429-z
PubMed Abstract | CrossRef Full Text | Google Scholar
47. Gai Tobe R, Islam MT, Yoshimura Y, Hossain J. Strengthening the community support group to improve maternal and neonatal health seeking behaviors: a cluster-randomized controlled trial in satkhira district, Bangladesh. PloS One. (2019) 14(2):e0212847. doi: 10.1371/journal.pone.0212847
PubMed Abstract | CrossRef Full Text | Google Scholar
48. Okawa S, Gyapong M, Leslie H, Shibanuma A, Kikuchi K, Yeji F, et al. Effect of continuum-of-care intervention package on improving contacts and quality of maternal and newborn healthcare in Ghana: a cluster randomised controlled trial. BMJ open. (2019) 9(9):e025347. doi: 10.1136/bmjopen-2018-025347
PubMed Abstract | CrossRef Full Text | Google Scholar
49. Waiswa P, Pariyo G, Kallander K, Akuze J, Namazzi G, Ekirapa-Kiracho E, et al. Effect of the Uganda newborn study on care-seeking and care practices: a cluster-randomised controlled trial. Glob Health Action. (2015) 8(1):24584. doi: 10.3402/gha.v8.24584
PubMed Abstract | CrossRef Full Text | Google Scholar
50. Kikuchi K, Ansah EK, Okawa S, Enuameh Y, Yasuoka J, Nanishi K, et al. Effective linkages of continuum of care for improving neonatal, perinatal, and maternal mortality: a systematic review and meta-analysis. PloS One. (2015) 10(9):e0139288. doi: 10.1371/journal.pone.0139288
PubMed Abstract | CrossRef Full Text | Google Scholar
51. Khan MN, Harris ML, Loxton D. Assessing the effect of pregnancy intention at conception on the continuum of care in maternal healthcare services use in Bangladesh: evidence from a nationally representative cross-sectional survey. PloS one. (2020) 15(11):e0242729. doi: 10.1371/journal.pone.0242729
PubMed Abstract | CrossRef Full Text | Google Scholar
52. Obasola OI, Mabawonku I, Lagunju I. A review of e-health interventions for maternal and child health in sub-sahara Africa. Matern Child Health J. (2015) 19(8):1813–24. doi: 10.1007/s10995-015-1695-0
PubMed Abstract | CrossRef Full Text | Google Scholar
53. Coleman J, Black V, Thorson AE, Eriksen J. Evaluating the effect of maternal mHealth text messages on uptake of maternal and child health care services in South Africa: a multicentre cohort intervention study. Reprod Health. (2020) 17(1):1–9. doi: 10.1186/s12978-020-01017-3
PubMed Abstract | CrossRef Full Text | Google Scholar
54. Tobe RG, Haque SE, Ikegami K, Mori R. Mobile-health tool to improve maternal and neonatal health care in Bangladesh: a cluster randomized controlled trial. BMC Pregnancy Childbirth. (2018) 18(1):1–7. doi: 10.1186/s12884-017-1633-9
PubMed Abstract | CrossRef Full Text | Google Scholar
55. Bishanga DR, Massenga J, Mwanamsangu AH, Kim Y-M, George J, Kapologwe NA, et al. Women’s experience of facility-based childbirth care and receipt of an early postnatal check for herself and her newborn in northwestern Tanzania. Int J Environ Res Public Health. (2019) 16(3):481. doi: 10.3390/ijerph16030481
PubMed Abstract | CrossRef Full Text | Google Scholar
56. Emiru AA, Alene GD, Debelew GT. Women’s retention on the continuum of maternal care pathway in west gojjam zone, Ethiopia: multilevel analysis. BMC Pregnancy Childbirth. (2020) 20(1):1–14. doi: 10.1186/s12884-020-02953-5
CrossRef Full Text | Google Scholar
57. Camara BS, Benova L, Delvaux T, Sidibé S, El Ayadi AM, Grietens KP, et al. Women’s progression through the maternal continuum of care in Guinea: evidence from the 2018 Guinean demographic and health survey. Trop Med Int Health. (2021) 26(11):1446–61. doi: 10.1111/tmi.13661
PubMed Abstract | CrossRef Full Text | Google Scholar
58. Amin R, Shah NM, Becker S. Socioeconomic factors differentiating maternal and child health-seeking behavior in rural Bangladesh: a cross-sectional analysis. Int J Equity Health. (2010) 9(1):1–11. doi: 10.1186/1475-9276-9-9
PubMed Abstract | CrossRef Full Text | Google Scholar
59. Fenny AP, Asante FA, Enemark U, Hansen KS. Malaria care seeking behavior of individuals in Ghana under the NHIS: are we back to the use of informal care? BMC public Health. (2015) 15(1):1–8. doi: 10.1186/s12889-015-1696-3
PubMed Abstract | CrossRef Full Text | Google Scholar
60. Larsen A, Exavery A, Phillips JF, Tani K, Kanté AM. Predictors of health care seeking behavior during pregnancy, delivery, and the postnatal period in rural Tanzania. Matern Child Health J. (2016) 20(8):1726–34. doi: 10.1007/s10995-016-1976-2
PubMed Abstract | CrossRef Full Text | Google Scholar
61. Målqvist M, Yuan B, Trygg N, Selling K, Thomsen S. Targeted interventions for improved equity in maternal and child health in low-and middle-income settings: a systematic review and meta-analysis. PLoS One. (2013) 8(6):e66453. doi: 10.1371/journal.pone.0066453
CrossRef Full Text | Google Scholar
62. Haider MR, Rahman MM, Moinuddin M, Rahman AE, Ahmed S, Khan MM. Impact of maternal and neonatal health initiatives on inequity in maternal health care utilization in Bangladesh. PloS one. (2017) 12(7):e0181408. doi: 10.1371/journal.pone.0181408
PubMed Abstract | CrossRef Full Text | Google Scholar
63. Pulok MH, Uddin J, Enemark U, Hossin MZ. Socioeconomic inequality in maternal healthcare: an analysis of regional variation in Bangladesh. Health Place. (2018) 52:205–14. doi: 10.1016/j.healthplace.2018.06.004
PubMed Abstract | CrossRef Full Text | Google Scholar
64. Mia MN, Mahmood SS, Iqbal M, Bhuiya A, Pallikadavath S, Stones W. The Bangladesh maternal health voucher scheme: impact on completeness of antenatal care provision. J Biosoc Sci. (2022) 54(2):217–24. doi: 10.1017/S0021932020000784
PubMed Abstract | CrossRef Full Text | Google Scholar
65. Najnin N, Bennett CM, Luby SP. Inequalities in care-seeking for febrile illness of under-five children in urban Dhaka, Bangladesh. J Health Popul Nutr. (2011) 29(5):523. doi: 10.3329/jhpn.v29i5.8907
PubMed Abstract | CrossRef Full Text | Google Scholar
66. Chen LC, Huq E, d’Souza S. Sex bias in the family allocation of food and health care in rural Bangladesh. Popul Dev Rev. (1981) 7(1):55–70. doi: 10.2307/1972764
CrossRef Full Text | Google Scholar
67. Winch PJ, Alam MA, Akther A, Afroz D, Ali NA, Ellis AA, et al. Local understandings of vulnerability and protection during the neonatal period in sylhet district, Bangladesh: a qualitative study. Lancet. (2005) 366(9484):478–85. doi: 10.1016/S0140-6736(05)66836-5
PubMed Abstract | CrossRef Full Text | Google Scholar
68. Sasaki S, Fujino Y, Igarashi K, Tanabe N, Muleya CM, Suzuki H. Access to a health facility and care-seeking for danger signs in children: before and after a community-based intervention in Lusaka, Zambia. Trop Med Int Health. (2010) 15(3):312–20. doi: 10.1111/j.1365-3156.2009.02460.x
PubMed Abstract | CrossRef Full Text | Google Scholar
70. Buor D. Analysing the primacy of distance in the utilization of health services in the ahafo-ano south district, Ghana. Int J Health Plann Manage. (2003) 18(4):293–311. doi: 10.1002/hpm.729
PubMed Abstract | CrossRef Full Text | Google Scholar
71. Kozuki N, Guenther T, Vaz L, Moran A, Soofi SB, Kayemba CN, et al. A systematic review of community-to-facility neonatal referral completion rates in Africa and Asia. BMC Public Health. (2015) 15(1):1–13. doi: 10.1186/s12889-015-2330-0
PubMed Abstract | CrossRef Full Text | Google Scholar
72. Save The Children. Bangladesh: national newborn health situation analysis report 2014. Save The Children and Government of Bnagladesh (2016).
73. icddr,b and Save The Children. MaMoni MNCSP: Health Facility Readiness Assessment Survey: Baseline Report, July 2020, (Unpublished) (2020).
74. Rahman AE, Herrera S, Rubayet S, Banik G, Hasan R, Ahsan Z, et al. Managing possible serious bacterial infection of young infants where referral is not possible: lessons from the early implementation experience in Kushtia district learning laboratory, Bangladesh. PloS One. (2020) 15(5):e0232675. doi: 10.1371/journal.pone.0232675
PubMed Abstract | CrossRef Full Text | Google Scholar
75. Bogale TN, Worku AG, Yalew AW, Bikis GA, Tigabu Kebede Z. Mothers treatment seeking intention for neonatal danger signs in northwest Ethiopia: a structural equation modeling. Plos One. (2018) 13(12):e0209959. doi: 10.1371/journal.pone.0209959
PubMed Abstract | CrossRef Full Text | Google Scholar
76. Ekwochi U, Ndu IK, Osuorah CD, Amadi OF, Okeke IB, Obuoha E, et al. Knowledge of danger signs in newborns and health seeking practices of mothers and care givers in Enugu state, south-east Nigeria. Ital J Pediatr. (2015) 41(1):1–7. doi: 10.1186/s13052-015-0127-5
PubMed Abstract | CrossRef Full Text | Google Scholar
77. Ekwochi U, Ndu IK, Osuorah CD, Onah KS, Obuoha E, Odetunde OI, et al. Delays in healthcare delivery to sick neonates in Enugu south-east Nigeria: an analysis of causes and effects. J Public Health (Bangkok). (2016) 38(2):e171–e7. doi: 10.1093/pubmed/fdv092
CrossRef Full Text | Google Scholar
78. Dongre AR, Deshmukh PR, Garg BS. Awareness and health care seeking for newborn danger signs among mothers in peri-urban Wardha. Indian J Pediatr. (2009) 76(7):691–3. doi: 10.1007/s12098-009-0106-1
PubMed Abstract | CrossRef Full Text | Google Scholar
79. Choi Y, El Arifeen S, Mannan I, Rahman S, Bari S, Darmstadt G, et al. Can mothers recognize neonatal illness correctly? Comparison of maternal report and assessment by community health workers in rural Bangladesh. Trop Med Int Health. (2010) 15(6):743–53. doi: 10.1111/j.1365-3156.2010.02532.x
PubMed Abstract | CrossRef Full Text | Google Scholar
80. Ministry of Health and Family Welfare (MOHFW). National neonatal health strategy and guidelines for Bangladesh. Ministry of Health and Family Welfare, Government of the People’s Republic of Bnagladessh (2009).
81. World Health Organization. WHO Recommendations on postnatal care of the mother and newborn. World Health Organization (2014).
82. Baqui AH, Arifeen SE, Rosen HE, Mannan I, Rahman SM, Al-Mahmud AB, et al. Community-based validation of assessment of newborn illnesses by trained community health workers in sylhet district of Bangladesh. Trop Med Int Health. (2009) 14(12):1448–56. doi: 10.1111/j.1365-3156.2009.02397.x
PubMed Abstract | CrossRef Full Text | Google Scholar
83. Darmstadt GL, Baqui AH, Choi Y, Bari S, Rahman SM, Mannan I, et al. Validation of a clinical algorithm to identify neonates with severe illness during routine household visits in rural Bangladesh. Arch Dis Child. (2011) 96(12):1140–6. doi: 10.1136/archdischild-2011-300591
PubMed Abstract | CrossRef Full Text | Google Scholar
84. Killewo J, Anwar I, Bashir I, Yunus M, Chakraborty J. Perceived delay in healthcare-seeking for episodes of serious illness and its implications for safe motherhood interventions in rural Bangladesh. J Health Popul Nutr. (2006) 24(4):403. doi: 10.3329/JHPN.V24I4.692
PubMed Abstract | CrossRef Full Text | Google Scholar
85. Werner C, Schermelleh-Engel K. Structural equation modeling: advantages, challenges, and problems. Introduction to structural equation modeling with LISREL. (2009).
Google Scholar
86. Jemberia MM, Berhe ET, Mirkena HB, Gishen DM, Tegegne AE, Reta MA. Low level of knowledge about neonatal danger signs and its associated factors among postnatal mothers attending at Woldia general hospital, Ethiopia. Matern Health Neonatol Perinatol. (2018) 4(1):1–8. doi: 10.1186/s40748-018-0073-5
PubMed Abstract | CrossRef Full Text | Google Scholar
link





